What Is Menopause? Symptoms, Stages, Age, and Treatment
After fifteen years and more than 5,000 patient visits a year, I can tell you the most common sentence I hear in my exam room. It isn't about hot flashes. It's this: "Dr. Kashyap, I don't feel like myself anymore , and nobody can tell me why."
If that sounds familiar, I want you to know two things before you read another word: you are not imagining it, and you do not have to live with it.
There is much more to menopause than hot flashes. In this guide, I'll walk you through what menopause actually is, the stages and ages, the full picture of symptoms (including the ones nobody warns you about), how long it lasts, and the treatment options that actually work , the same way I explain it to the women who sit across from me every day.
|
Menopause at a Glance
|
|
|
Average age of menopause (US)
|
About 52 (range 45–55 is typical), per the National Institute on Aging1
|
|
When perimenopause usually begins
|
Early-to-mid 40s, sometimes earlier
|
|
How long symptoms last
|
Median of about 7.4 years, per the SWAN study2,longer for many women
|
|
Most common symptoms I see
|
Hot flashes, brain fog, vaginal dryness
|
|
Official definition of menopause
|
12 consecutive months without a period
|
|
Can it be treated?
|
Yes , hormonal, non-hormonal, and lifestyle options all exist
|
What Is Menopause and What Causes It?
Menopause is the point when your menstrual periods stop permanently, officially, when you've gone 12 consecutive months without a period. As the name suggests, menopause means the pausing of menstrual cycles.
But here's what that definition leaves out, and what I want every woman to understand: menopause happens because your ovaries gradually stop making hormones that have been doing critically important work in your body for decades.
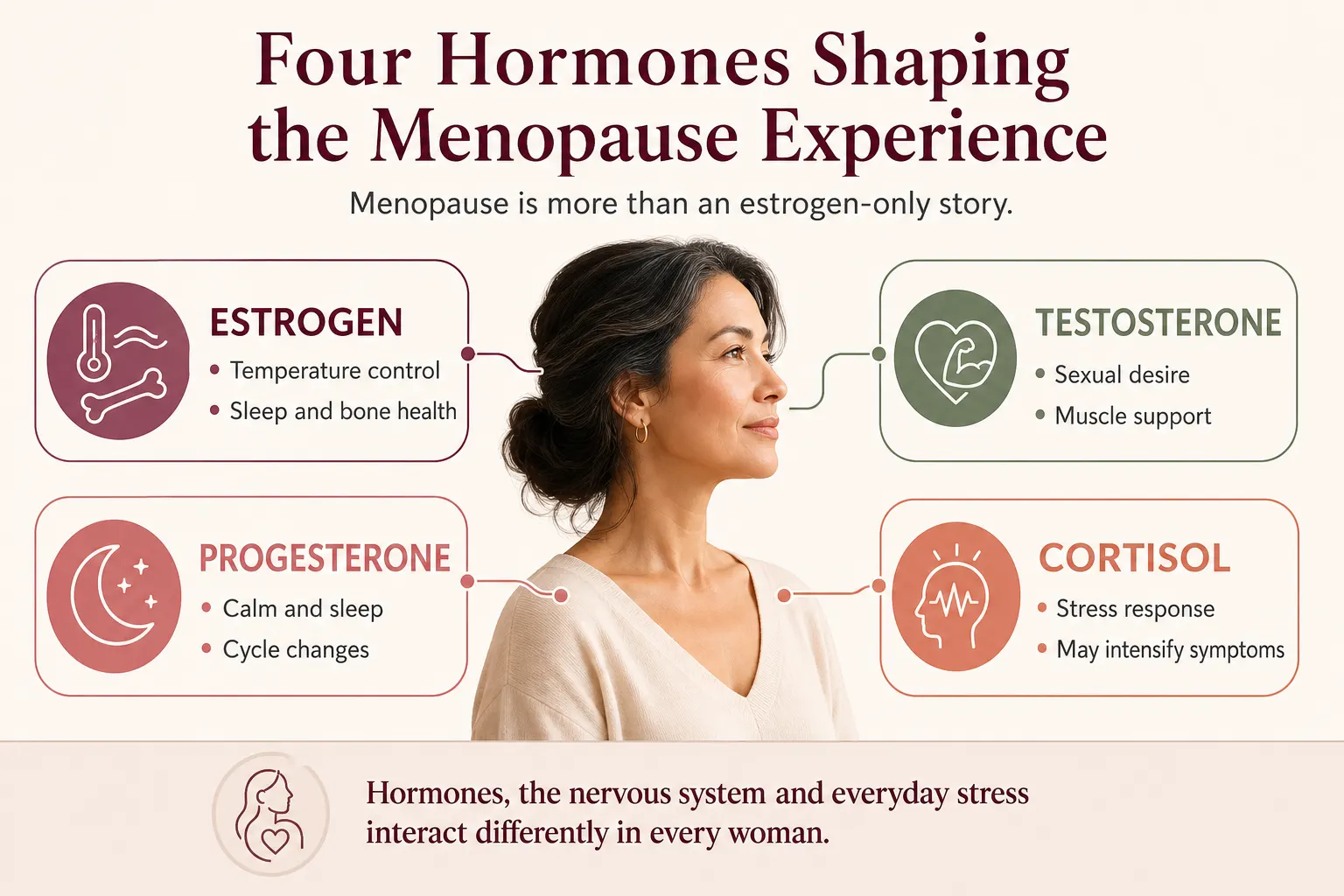
Most people , including, frankly, many doctors , talk about menopause as a single-hormone, estrogen-only story. In my practice, I think about it more broadly: several hormones shift together during this transition, and stress biology can influence how strongly any individual woman experiences her symptoms.
- Estrogen: When it declines, you get hot flashes, night sweats, and difficulty sleeping. Estrogen is also critical for maintaining your bones.
- Progesterone: This hormone naturally supports calm and sleep. As it fluctuates and declines, sleep quality often suffers, and poor sleep can in turn contribute to the fatigue and "brain fog" so many women describe. Women tell me, "I cannot think straight. I cannot remember things which I used to." ,and disrupted sleep is very often a major driver of that experience.
- Testosterone: Yes, women make testosterone, and yes, it plays a role in desire. I remind patients of this every single week: it is not just a male hormone. Some evidence also suggests a connection between testosterone decline and changes in muscle and fat,though this relationship is less firmly established, and testosterone therapy is not a guaranteed fix for weight or muscle concerns.
- Cortisol : Your body's main stress hormone. Cortisol is not technically one of the hormones that defines menopause, and menopause itself does not directly raise cortisol. But many women are going through this hormonal transition at exactly the same time their life , caregiving, careers, aging parents, poor sleep , is asking the most of them. That combination of stress and aging can shape how strongly menopause symptoms are felt, which is why I never treat menopause as a hormone-only conversation.
Menopause isn't an estrogen deficiency to be patched. It's what I call a dynamic state of neuroendocrine recalibration , your hormonal system, your nervous system, and your life circumstances are all adjusting together. My job, and the job of any good menopause doctor, is to interpret the signal, not just silence the symptom.
|
DR. KASHYAP'S TIP
Start a simple symptom-and-period diary today , dates of your periods, sleep quality, mood, and any new symptoms. Six months of notes tells me more in one visit than an hour of trying to remember. Your phone's notes app is enough.
|
Perimenopause vs. Menopause vs. Postmenopause: The 3 Stages
One of the biggest sources of confusion I see is the difference between perimenopause and menopause. Let me make it simple:
|
Stage
|
What It Means
|
Typical Age
|
What You May Notice
|
|
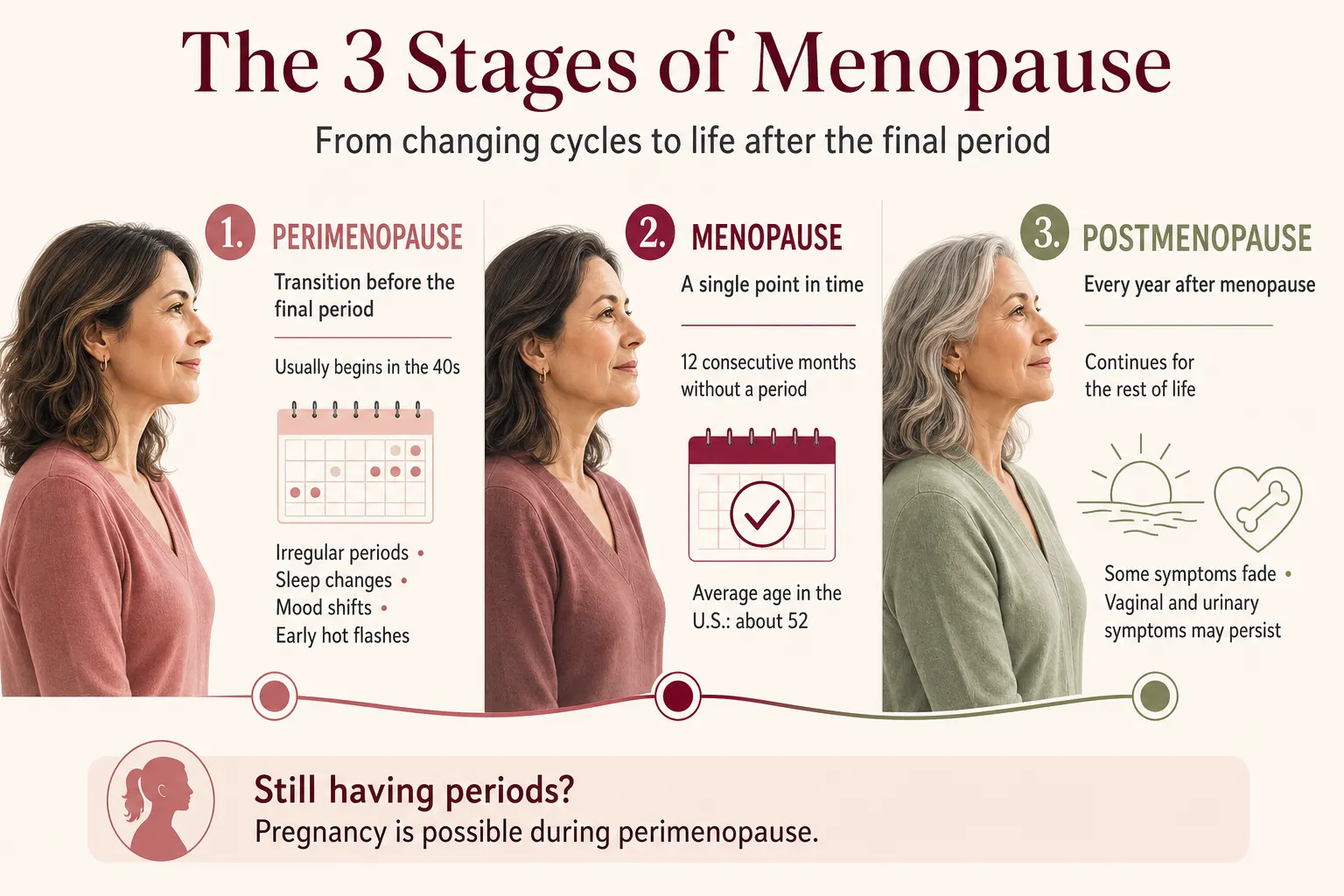
Perimenopause
|
The transition years before your final period. Hormones fluctuate unpredictably.
|
Often begins in your early-to-mid 40s
|
Irregular periods, new sleep problems, mood swings, early hot flashes, brain fog
|
|
Menopause
|
The single point in time: 12 months with no period
|
Average age 52 in the US
|
Symptoms often peak around this window
|
|
Postmenopause
|
Every year after that point ,for the rest of your life
|
50s onward
|
Some symptoms fade; others (like vaginal dryness) can persist or worsen without treatment
|
The key difference between perimenopause and menopause symptoms? In perimenopause, you still have periods , they're just erratic, and symptoms come in waves as hormones swing up and down. In menopause and postmenopause, hormone levels settle at a lower baseline, so symptoms become more constant.
Here's the part most women miss: once your periods stop, you don't "finish" menopause and go back to normal. You remain postmenopausal for the rest of your life. Whether the symptoms fade , and which ones ,varies from woman to woman. That's exactly why I tell patients not to wait it out.
|
QUICK QUESTION
Can you get pregnant during perimenopause?
Yes. As long as you are still having periods ,even irregular ones , pregnancy is possible. Continue contraception until menopause is confirmed: 12 full months without a period.
|
What Age Does Menopause Start?
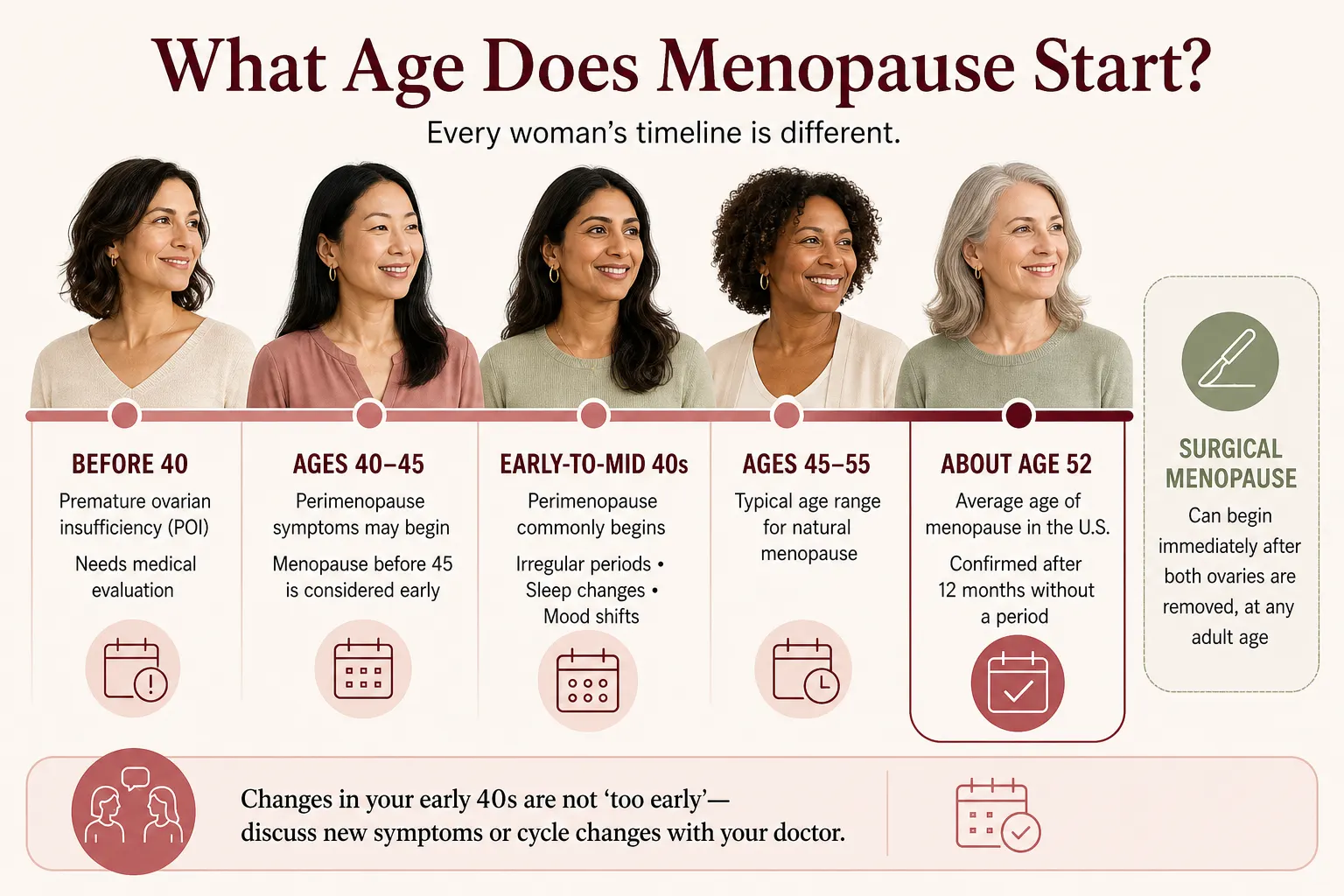
The average age of menopause in the United States is about 52, according to the National Institute on Aging.1 But I want to be very clear about something I see constantly in my clinic: some women start experiencing changes much sooner than others.
Perimenopause typically begins in your early 40s , sometimes earlier. So if you're 44 or 47 and your periods are shifting, your sleep has fallen apart, and you feel like a stranger in your own body, you are not "too young for this." You may be right on schedule.
A quick guide to ages:
- Symptoms at 40–45: Very often perimenopause. Don't let anyone dismiss you.
- Symptoms at 47–50: This is the heart of the transition for most women.
- Menopause before 45 is considered early menopause; before 40 is premature menopause (also called premature ovarian insufficiency). Both deserve a thorough medical workup causes can include genetics, autoimmune conditions, surgery, chemotherapy, or smoking , and both carry long-term bone and heart implications that make treatment especially important.
- Surgical menopause: If your ovaries are removed, menopause begins immediately, often with more intense symptoms because the hormone drop is sudden rather than gradual.
So, I recommend that every woman begin a midlife awareness plan in her early 40s ,not after her last period. Starting early lets us slow or soften many of these changes and protect your bones and heart while there's still a window to act.
|
DR. KASHYAP'S TIP
Turning 40? Ask your doctor for a baseline: blood pressure, lipids, blood sugar, vitamin D, and thyroid. Knowing your numbers before the transition makes every later decision smarter.
|
Menopause Symptoms: The Complete List (Beyond Hot Flashes)
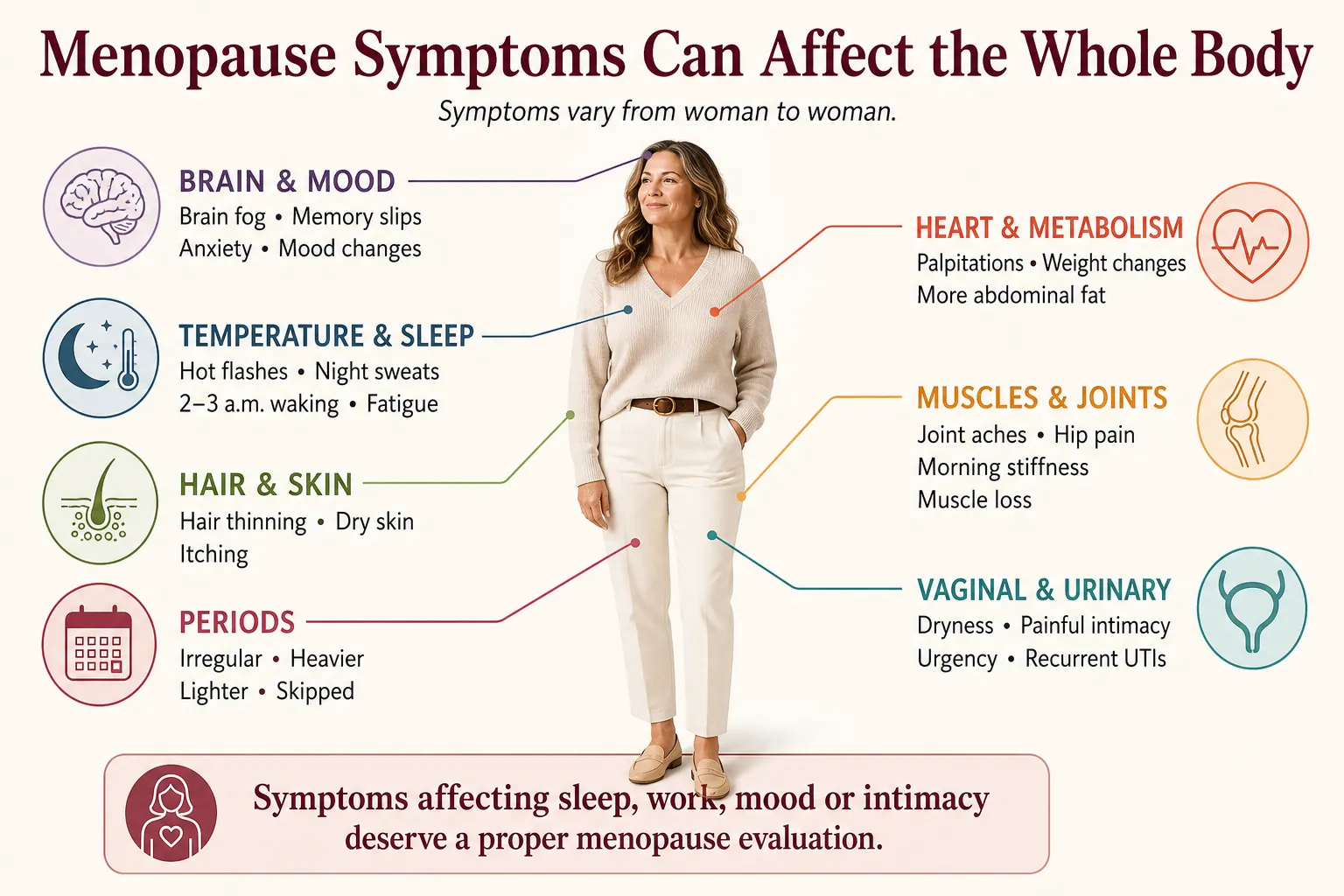
You may have seen viral lists of "34 symptoms of menopause", or even 50 or 100. The truth is, because these hormones touch nearly every system in your body, the list of possible symptoms is long. But after thousands of patients, I can tell you the three I see most often: hot flashes, foggy thinking, and vaginal dryness. Everything else clusters around them.
Here is the full picture, organized the way I assess it in my clinic.
Hot Flashes and Night Sweats (Vasomotor Symptoms)
Doctors call these vasomotor symptoms, and here's what's actually happening: declining estrogen confuses the brain's internal thermostat, which starts overreacting to tiny temperature changes as if they were emergencies. Up to 80% of women experience them, according to a research summary from the SWAN study3, making this the most recognized symptom of menopause , though, as you'll see, far from the only one. What they typically look like:
- A sudden wave of heat rising through the chest, neck, and face , often out of nowhere
- Flushing, a racing heart, and sweating, sometimes followed by chills as the wave passes
- Night sweats that soak your nightwear and sheets, jolting you awake
- Episodes lasting one to five minutes, anywhere from a few times a week to many times a day
- Common triggers: warm rooms, alcohol, caffeine, spicy food, and , tellingly , stress
They're more than a nuisance. Night after night of fragmented sleep spills into mood, memory, weight, and everything else , which is why I treat them seriously, not as something to fan away.
Brain Fog, Memory, and Concentration
My patients describe this one best: "I cannot think straight. I cannot remember things which I used to." Research published in JAMA4 suggests roughly 40–60% of women in the menopause transition notice cognitive changes. Several things tend to converge here: hormonal fluctuations, fragmented sleep, and the accumulated effect of stress , and poor sleep in particular is one of the biggest contributors to the foggy, slowed-down feeling women describe. If any of these sound familiar, you're in very large company:
- Walking into a room and forgetting why you came
- Losing words mid-sentence,the name, the date, the thing on the tip of your tongue
- Reading the same page twice because nothing stuck the first time
- Missing appointments or details you'd never have missed before
- Feeling mentally slower in meetings or conversations , and quietly scared about it
Here's what I want you to hold onto: menopause brain fog is not dementia. For the vast majority of women, performance stays within the normal range and improves after the transition. It is frightening, but it is usually temporary , and treatable.
Sleep Problems
Midlife insomnia is one of the most life-draining symptoms I treat, and one of the most responsive to the right plan. Night sweats are one culprit, and shifting progesterone levels are commonly linked with sleep disruption as well. The pattern my patients report:
- Trouble falling asleep, even when you're exhausted
- The infamous 2–3 a.m. waking,eyes open, mind racing, sleep gone
- Night-sweat wake-ups that require changing clothes or sheets
- Waking unrefreshed no matter how many hours you logged
Weight Gain and the "Menopause Belly"
"I'm eating the same, exercising the same, and the weight goes straight to my middle." I hear this almost daily, usually delivered with guilt , and the guilt is misplaced, because the science backs these women up. What's actually happening in the transition:
- The rate of fat gain has been shown to increase, while lean muscle mass tends to decline, according to a SWAN cohort study published in JCI Insight5
- Deep belly (visceral) fat tends to accumulate more in the years around the final period , a pattern that appears at least partly independent of aging alone5
- The scale can stay the same while your body composition and waistline change, muscle out, fat in
- Bloating adds insult, fluctuating through the day as hormones and digestion shift
Declining estrogen plays a role in this shift, and testosterone is suggested to be involved as well, though the evidence on testosterone's exact contribution is still developing. The answer is not starving yourself, it's strength training to protect muscle, adequate protein, stress regulation, and in the right candidates, hormonal support.
Joint Pain, Hip Pain, and Body Aches
One of the most under-recognized symptom groups , what researchers now call the musculoskeletal syndrome of menopause. Estrogen is anti-inflammatory and supports your tendons, cartilage, and muscle; as it falls, all that quiet protection fades at once. If your joints "aged overnight" in your late 40s, this may be the missing explanation your doctors haven't connected. The classic pattern:
- Morning stiffness,joints feel rusted shut for the first 20–30 minutes of the day
- Migrating aches,knees one week, fingers the next, shoulders after that
- Outer-hip pain at night, worse when lying on that side
- Frozen shoulder,a progressively stiff, locked shoulder that strikes women aged 40–60 far more than anyone else
- Stiffness after sitting that takes a few steps to "unlock"
Hair Thinning and Skin Changes
Estrogen supports hair density and skin collagen. As it falls, many women notice thinning hair, more shedding, drier skin, and new wrinkles. There are real treatment options here , from addressing the hormonal root to targeted topical and nutritional support , so please don't accept "that's just aging."
Vaginal Dryness, Painful Sex, and Urinary Changes
This is the symptom cluster women suffer through in silence , mentioned last in my exam room, hand on the doorknob, if it's mentioned at all. Estrogen loss thins the vaginal tissue and changes the urinary tract, and the medical name for the whole picture is genitourinary syndrome of menopause (GSM). The North American Menopause Society6 reports that GSM affects approximately 27% to 84% of postmenopausal women , and most of them never bring it up. What it includes:
- Vaginal dryness, burning, or itching that doesn't resolve
- Painful sex,many women describe it to me as feeling "like sandpaper"
- Recurrent urinary tract infections, one after another
- Urgency and leaks,suddenly needing to go, or leaking with coughs and laughs
Two things to remember. Unlike hot flashes, these symptoms do not fade on their own, they progress without treatment. And they are among the most treatable symptoms in all of menopause medicine. Don't suffer in silence.
Mood Changes, Anxiety, and Irritability
Hormonal shifts can affect brain chemistry, and the life stage amplifies it. If your mood feels foreign to you, it deserves medical attention , not just "self-care."
|
QUICK QUESTION
Can menopause cause anxiety?
Hormonal fluctuation is commonly linked with new or worsening anxiety during the transition , even in women who have never experienced it before. It is treatable, so do mention it to your doctor.
|
Other symptoms my patients report
Bloating, heart palpitations, dizziness, headaches and migraines, nausea, breast tenderness, dry eyes, itchy skin, burning mouth, and changes in body odor. Strange? Yes. Connected to hormones? Very often, yes.
Menopause Symptoms Checklist: A Quick Self-Check
Tick what applies to you over the last 3 months. If you check 3 or more, your symptoms deserve a proper menopause evaluation , print this list or screenshot it, and bring it to your appointment.
☐ Hot flashes or night sweats
☐ Sleep problems,trouble falling asleep or 2–3 a.m. waking
☐ Brain fog, word-finding trouble, or memory slips
☐ Irregular, heavier, or skipped periods
☐ New weight gain around the middle despite no change in habits
☐ Joint aches, hip pain, or morning stiffness
☐ Vaginal dryness, discomfort, or pain with intimacy
☐ Low desire or change in sexual response
☐ New anxiety, irritability, or mood swings
☐ Hair thinning or drier skin
☐ Fatigue that rest doesn't fix
☐ Recurrent urinary infections or new leakage
The Cortisol Connection: Why Stress Biology Matters in Menopause
One part of menopause that is often overlooked is cortisol, the body's main stress hormone. Cortisol is not bad, we need it. It helps the body respond to pressure, danger, deadlines, and sudden demands. The problem begins when the body stays in that "alert mode" for too long.
During menopause, this matters even more. At the same time estrogen, progesterone, and testosterone are shifting, many women are also carrying years of stress from work, family responsibilities, caregiving, poor sleep, and emotional overload. The body is trying to adjust hormonally while also managing a high stress load.
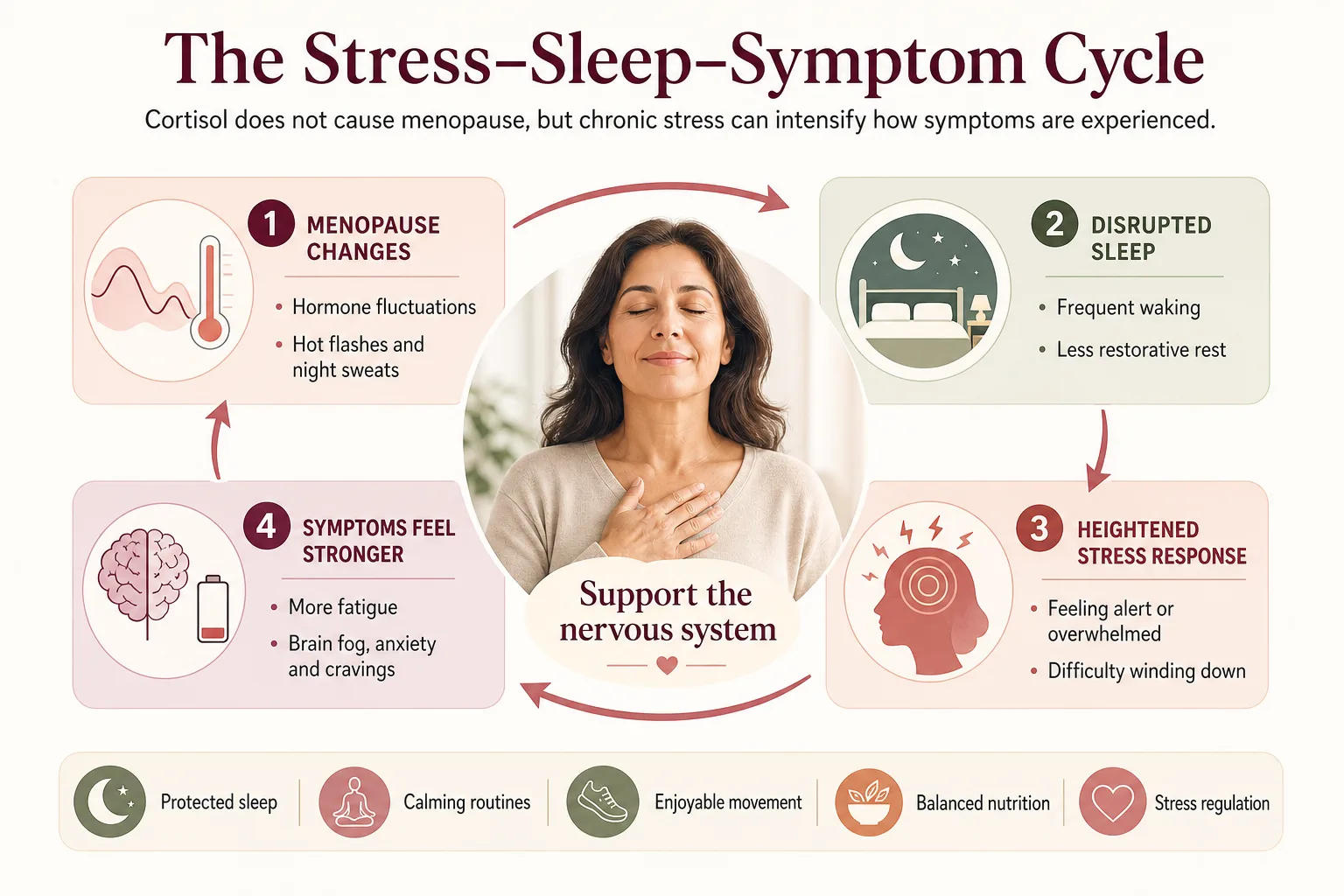
Even when two women have similar lab results, their menopause experience can feel very different. One may have mild symptoms, while another may struggle with intense hot flashes, poor sleep, anxiety, weight gain, or brain fog. Hormones are part of the picture, but stress biology can influence how strongly those symptoms are felt.
So, I do not look at menopause as a prescription-only problem. Hormone therapy, when appropriate, can be very helpful, but it works best when we also support the nervous system. Breathwork, protected sleep, calming bedtime routines, enjoyable movement, nutrition, and stress regulation are not "extras." They are part of a complete menopause care plan.
|
DR. KASHYAP'S TIP
Try the 4–6 breath tonight: inhale for 4 counts, exhale slowly for 6, for two minutes before bed. To be clear,breathing exercises are not a treatment for hot flashes, but a longer exhale helps calm the stress response, and many of my patients find it helps them settle at night.
|
How Long Does Menopause Last?
The question every patient asks me, so let me answer it directly.
Symptoms last a median of about 7.4 years, according to the landmark SWAN study2 (the Study of Women's Health Across the Nation), which followed thousands of American women through the transition. For some women it's shorter; for many it's longer, symptoms commonly persist 4–5 years after the final period, and women whose symptoms start early in perimenopause can experience them for more than a decade. In my own practice, I tell women the realistic range is anywhere from six or seven years to ten, even fifteen.
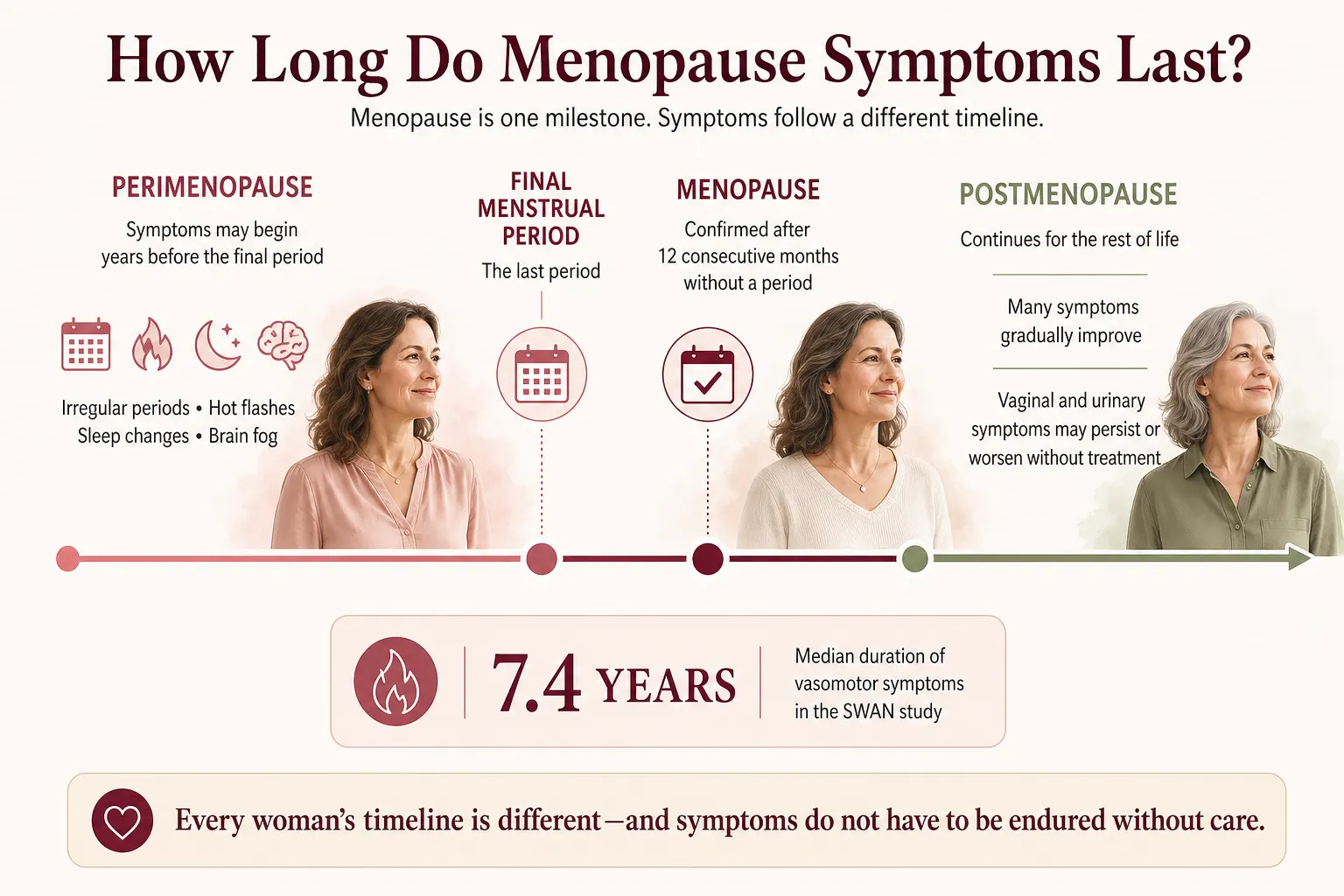
What signals the end of menopause? Technically, menopause itself is a single milestone , 12 consecutive months without a period. After that, you are postmenopausal for life. What people usually mean by "the end" is the end of symptoms, and that tapering looks different for everyone. Hot flashes typically fade over time. But , and this matters , some symptoms, especially vaginal dryness and urinary changes, do not fade. They persist or progress unless treated.
Do menopause symptoms go away? Many do, gradually. Some don't. And none of them have to be endured in the meantime. The "grit your teeth and wait" approach costs women years of sleep, intimacy, confidence, and health, for nothing. There is no medal for suffering through it.
|
QUICK QUESTION , Is there a test that confirms menopause?
Usually not a single one. FSH blood levels swing widely in perimenopause, so in women over 45 the diagnosis is made from your symptoms and period history , not one lab number.
|
Menopause Myths vs. Facts
I spend a surprising amount of every week un-teaching myths. Here are the ones I hear most:
|
Myth
|
Fact
|
|
"Menopause is just hot flashes."
|
Hot flashes are one symptom of dozens. Brain fog, joint pain, sleep loss, mood changes, and vaginal symptoms are just as real , and just as treatable.
|
|
"Hormone therapy is dangerous for everyone."
|
For healthy women under 60 or within 10 years of menopause, benefits generally outweigh risks. It's individual , candidacy is what matters, not blanket fear.
|
|
"Testosterone is a male hormone."
|
Women make and need testosterone too , current evidence most clearly supports its role in desire, with muscle and metabolism effects suggested but less firmly established.
|
|
"Weight gain is inevitable, just eat less."
|
The biology shifts (muscle down, visceral fat up), so the strategy must shift: strength training, protein, sleep, and stress work , not starvation.
|
|
"Vaginal dryness is just part of aging."
|
It's a treatable medical condition (GSM). Low-dose vaginal estrogen is safe for the vast majority of women and works.
|
|
"You're too young for menopause at 44."
|
Perimenopause typically begins in the early-to-mid 40s. Age 44 with symptoms is right on schedule , and deserves attention, not dismissal.
|
Menopause Treatment Options: Hormonal, Non-Hormonal, and Natural
Here is my core philosophy, and I say it to every patient: menopausal hormone therapy is not a pill , it's a process. There is no one-size-fits-all menopause treatment. When a woman comes to me, I want to understand her: which symptoms are stealing her quality of life, what her health history allows, how she lives, eats, moves, and sleeps. Then we build a plan. Here are the tools in the toolbox.
Hormone Therapy (HRT/MHT): Done Right, It's Life-Changing
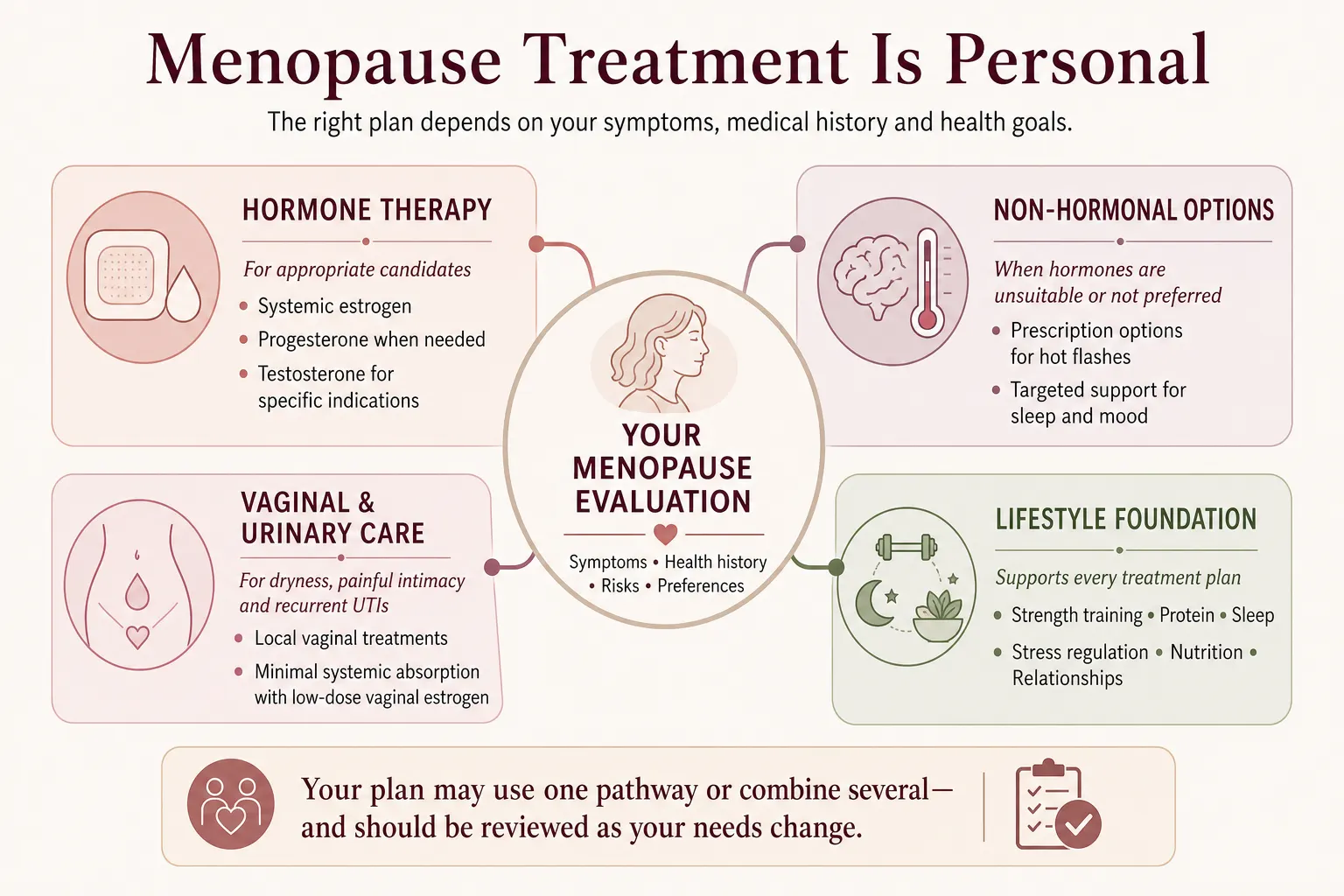
Hormone therapy remains the most effective treatment for hot flashes, night sweats, and vaginal symptoms, and it protects your bones. For healthy women under 60, or within 10 years of their final period, the benefits generally outweigh the risks. But the details matter enormously:
- Who needs individualized evaluation: women with hormone-sensitive cancers (such as certain breast or uterine cancers), a prior history of blood clots, liver disease, or certain cardiovascular conditions need a careful, individualized discussion before starting hormone therapy , this is not a flat "no," but it does mean extra care, and sometimes a different approach. For these women, we often lean on the excellent non-hormonal options below.
- Route matters. For many women, transdermal estrogen , delivered through the skin via patch, gel, or cream , offers safety advantages because it avoids first-pass liver metabolism, which is one pathway linked to increased clotting risk with oral estrogen. This is one of the more meaningful refinements in modern menopause care. And one of the lowest effective doses that controls your symptoms is always our goal.
- Progesterone,often taken as a pill, at night. If you have a uterus, progesterone protects it. Many women also notice better sleep when it's taken at bedtime,my patients often tell me they finally "sleep like a baby." Clinical trials support a sleep benefit with bedtime dosing (commonly 300 mg in studies), alongside improvement in night sweats.
- Testosterone,typically delivered through the skin, not by mouth. For postmenopausal women with low desire that distresses them (the medical term is HSDD), carefully dosed testosterone is the most evidence-based hormonal option specifically for this concern. We start low and monitor.
- Vaginal (local) estrogen deserves its own mention: for dryness, painful sex, and recurrent UTIs, low-dose vaginal estrogen works directly where it's needed with very minimal absorption into the rest of the body. It is safe for the vast majority of women,including many who can't use systemic hormones,and it is dramatically underused.
|
DR. KASHYAP'S TIP
Already on hormone therapy but still symptomatic? Don't quit,ask about the route, dose, and type before giving up. Many "HRT failures" I see are really dosing or delivery mismatches.
|
Non-Hormonal Prescription Options
If hormones aren't right for you, you are not out of options,and this field has finally advanced:
- Fezolinetant (Veozah),the first FDA-approved non-hormonal medication designed specifically for hot flashes, working on the brain's temperature-control center.
- Low-dose paroxetine,the FDA-approved SSRI option for hot flashes, also helpful when mood symptoms travel with them.
- Targeted medications for sleep, mood, and low desire, chosen for your specific picture.
Supplements and Natural Remedies: My Honest Take
Patients ask me about supplements daily, so let me be straight with you. Some botanicals,black cohosh, red clover,have mixed and inconsistent evidence for hot flashes; none of them is a reliable or proven treatment, and black cohosh shouldn't be used long-term or with liver disease. Adaptogens like ashwagandha show promise for stress and sleep, though menopause-specific data is limited.
What I focus on first is more fundamental: your hormones are made from raw materials. Green leafy vegetables, good fats (stop fearing fat,your hormones are built from it), vitamins, and minerals give your body what it needs to make the most of the hormones it still produces. Magnesium and vitamin D have particular roles in sleep, mood, and bone health. Supplements support a plan; they don't replace one.
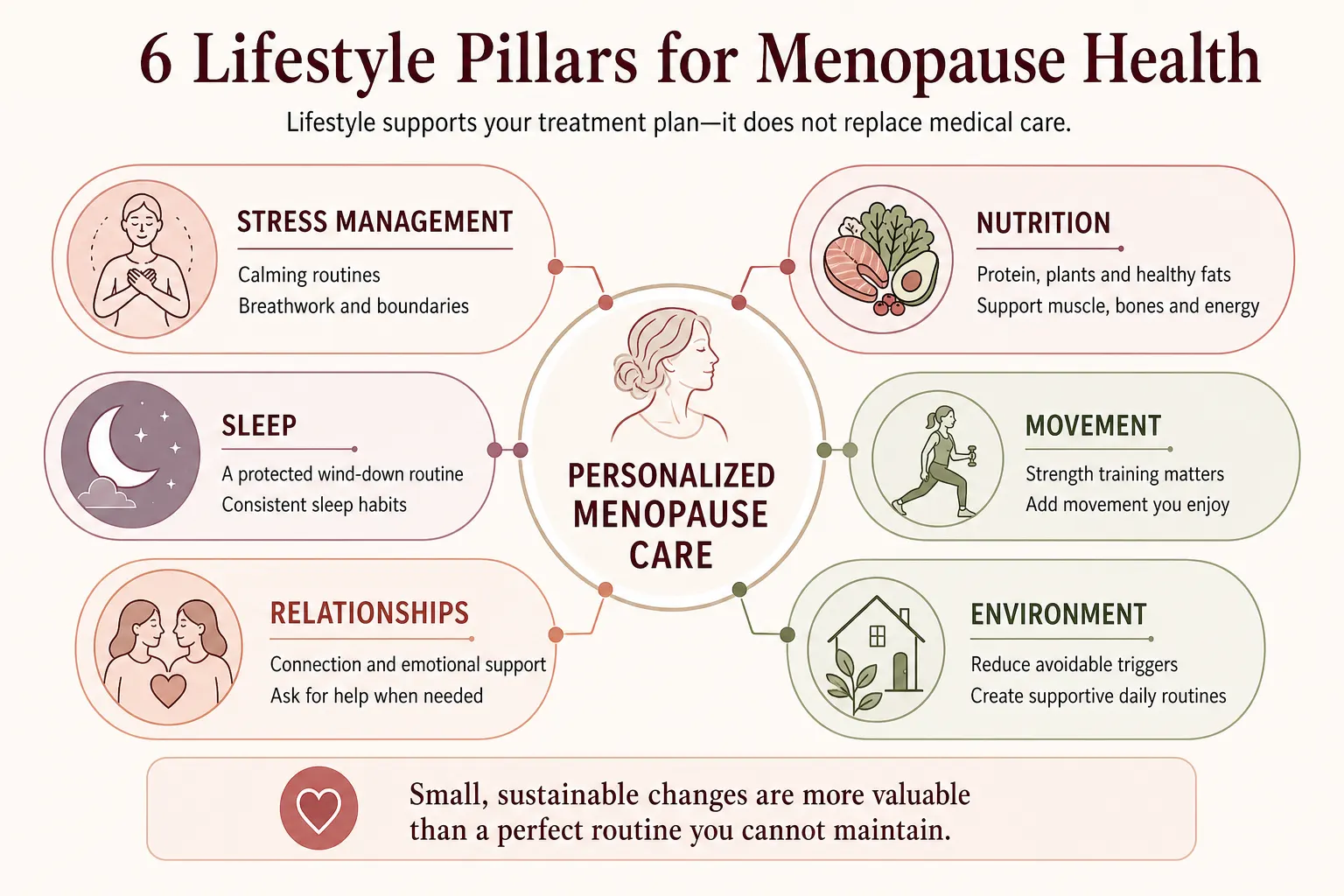
Lifestyle: The Foundation Everything Else Stands On
In my practice we build every plan on six pillars: stress management, nutrition, sleep, movement, relationships, and environment. Two I'll highlight because they change outcomes the most: strength training (to fight the muscle loss and belly-fat shift) and a real, protected wind-down routine at night (because no hormone can out-prescribe a phone in bed at midnight). And make your movement something fun,the best exercise plan is the one you'll actually keep doing.
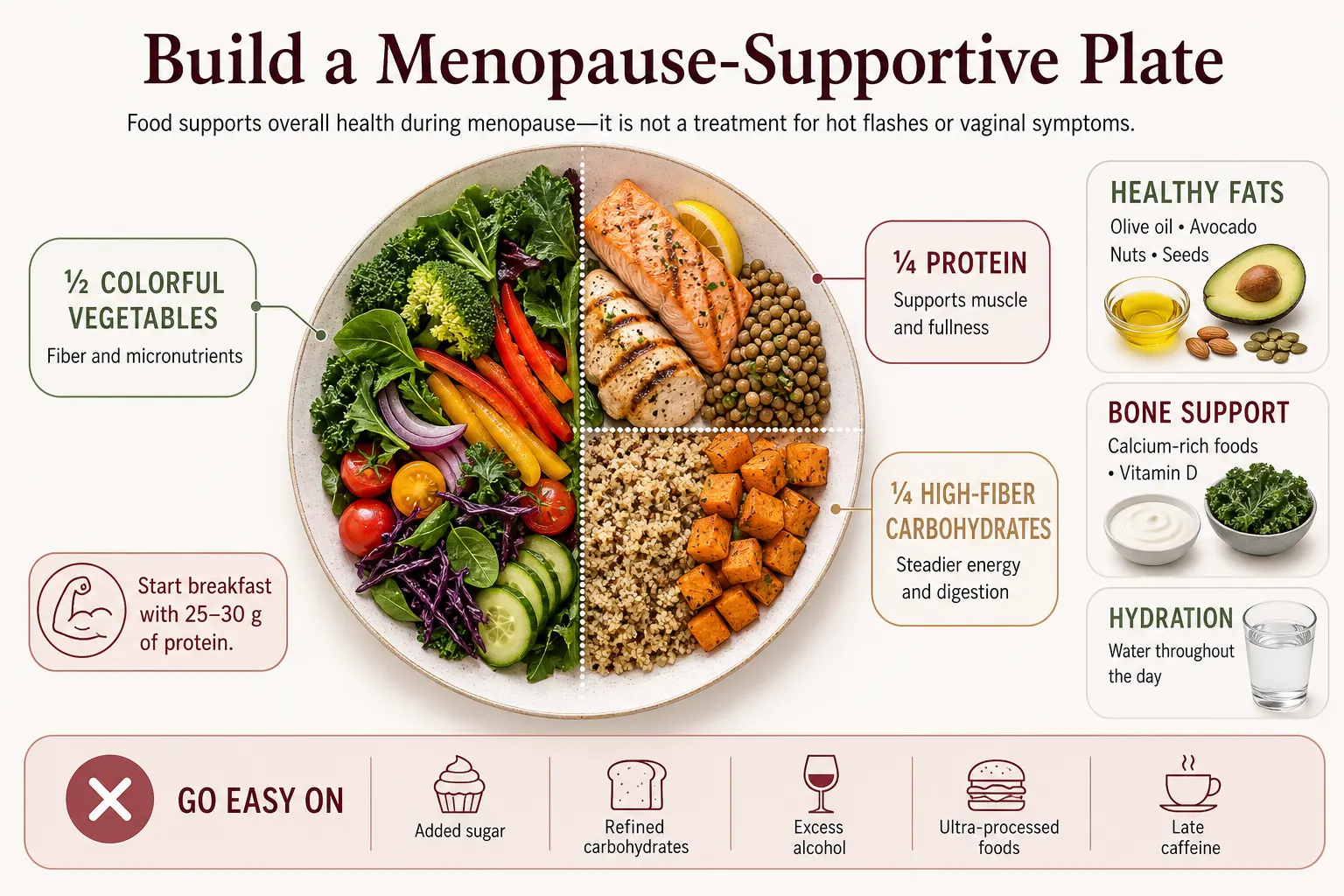
What to Eat During Menopause: Foods That Help, Foods That Don't
One honest note before the list: food supports your overall health during menopause,energy, digestion, muscle, bones, and weight. It is not a treatment for symptoms like hot flashes or vaginal dryness, and no single food will fix the transition. But the right plate makes every other part of your plan work better. Here's how I guide my patients:
|
Build Your Plate Around
|
Go Easy On
|
|
Protein at every meal,eggs, fish, chicken, Greek yogurt, lentils, tofu,to protect muscle
|
Added sugar and sweetened drinks,the most direct fuel for belly fat and energy crashes
|
|
Colorful vegetables and leafy greens,fiber, raw materials for hormone metabolism
|
Refined carbs,white bread, pastries, chips that spike blood sugar
|
|
Good fats,olive oil, avocado, nuts, fatty fish; your hormones are built from fat
|
Alcohol,disrupts sleep, worsens hot flashes for many women, and stores as belly fat
|
|
Calcium + vitamin D sources,dairy or fortified alternatives, for bones
|
Ultra-processed packaged foods,high salt (bloating) and industrial oils
|
|
Water through the day,supports energy and digestion
|
Late heavy meals and late caffeine,both sabotage already-fragile sleep
|
|
DR. KASHYAP'S TIP
The simplest upgrade I give patients: anchor breakfast with 25–30 grams of protein. It steadies blood sugar, cuts late-day cravings, and protects the muscle menopause is trying to take.
|
When to See a Menopause Specialist
- See a doctor,ideally one certified in menopause care,if:
- Your symptoms are interfering with sleep, work, mood, or intimacy
- You're under 45 and your periods are changing or stopping
- You have any bleeding after menopause (this always needs evaluation,promptly)
- You've been told "your labs are normal, it's just aging" but you know something is wrong
On that last point: a single FSH blood test is often unreliable during perimenopause because hormones fluctuate day to day. A persistently elevated FSH (typically above 30 IU/L alongside 12 months without a period) supports the diagnosis, but in most women over 45, menopause is diagnosed by your story and symptoms,not a lab number. A doctor who only treats the lab value is missing you.
And one more reminder I give every reader: symptoms such as postmenopausal bleeding, recurrent urinary infections, persistent bloating, unexplained weight loss, severe fatigue, or significant mood changes should always be medically evaluated,never assumed to be "just menopause."
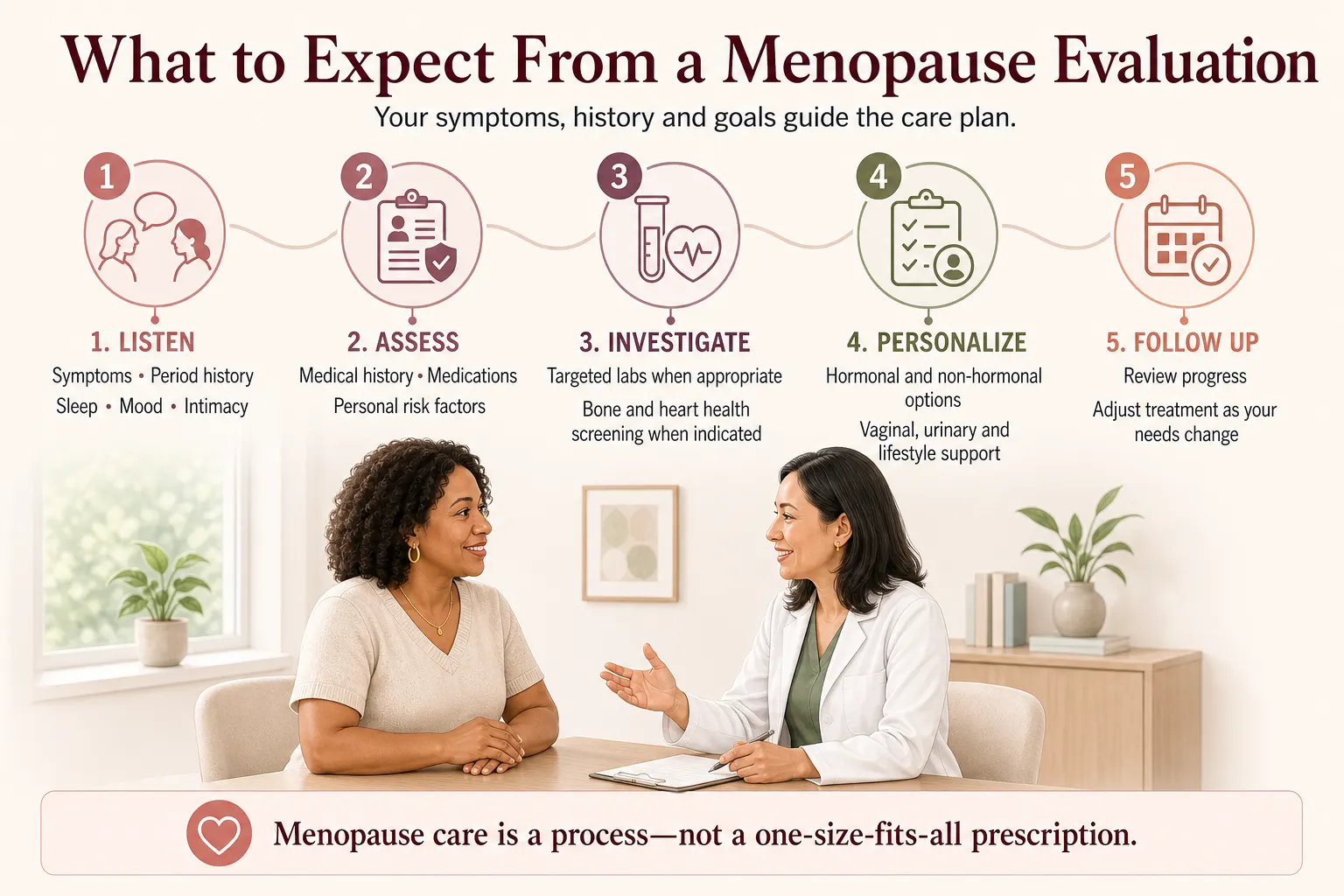
At Galleria Women's Health, my evaluation goes deeper: a detailed symptom and lifestyle assessment, comprehensive labs, bone density (DEXA), and heart-health screening where appropriate,because menopause is exactly the window when we can still protect your bones and your heart. Then we build your plan together and refine it at follow-up. That's the process.
If you're in the Henderson or Las Vegas area , I'd be honored to help you through this transition. Because here is the one thing I hope you take from this entire article: if you can't sleep, can't think straight, can't lose the weight, or can't enjoy intimacy,don't lose hope. Go and talk to the right person. Nobody should be living with these.
Book a consultation at Galleria Women's Health
Menopause Terms Explained: A Simple Glossary
Medical words shouldn't be a barrier to understanding your own body. Here's plain English for the terms you'll meet in this guide,and in your doctor's office:
- Estrogen — The primary female hormone, made mostly by the ovaries. It regulates your cycle and supports your bones, brain, skin, heart, and vaginal tissue. Its decline drives many menopause symptoms.
- Progesterone — A hormone that balances estrogen and prepares the uterus each cycle. Its fluctuation and decline are commonly linked with disrupted sleep, which can in turn contribute to fatigue and brain fog.
- Testosterone — Not just a male hormone,women produce it too, and current evidence most clearly supports its role in sexual desire. A connection to muscle and metabolism has been suggested, though this is less firmly established.
- Cortisol — Your body's main stress hormone. It is not one of the hormones that defines menopause, and menopause does not directly raise cortisol levels,but the stress and life demands many women carry during this transition can shape how intensely symptoms are experienced.
- Perimenopause — The transition years before your final period,often starting in the early-to-mid 40s,when hormones fluctuate and symptoms begin.
- Menopause — The single milestone of 12 consecutive months without a period. The average age in the US is about 52.
- Postmenopause — All the years after that milestone,the rest of your life. Some symptoms fade; bone and heart protection matter most here.
- Premature ovarian insufficiency (POI) — Menopause before age 40. It always deserves a full medical workup and usually treatment, because of long-term bone and heart effects.
- FSH (follicle-stimulating hormone) — A pituitary hormone that rises as the ovaries wind down. Useful as supporting evidence, but it fluctuates too much in perimenopause to be a yes/no test.
- Vasomotor symptoms (VMS) — The medical term for hot flashes and night sweats,caused by the brain's temperature thermostat misfiring as estrogen declines.
- GSM (genitourinary syndrome of menopause) — The umbrella term for vaginal dryness, painful sex, and urinary changes caused by estrogen loss in those tissues. It worsens without treatment,and it is very treatable.
- HRT / MHT (hormone replacement / menopausal hormone therapy) — Prescription estrogen,with progesterone if you have a uterus,used to treat symptoms and protect bone. Modern practice often favors the lowest effective dose, frequently delivered through the skin.
- Micronized progesterone — A body-identical form of progesterone taken as a capsule, usually at bedtime,it protects the uterus and is associated with improved sleep for many women.
- Visceral fat — Deep fat around the abdominal organs. It tends to increase around the final period and is linked to heart and metabolic risk,part of the story behind the "menopause belly."
- Osteopenia / Osteoporosis — Stages of bone loss. Estrogen protects bone; after menopause, loss accelerates,which is why we measure it.
- DEXA scan—A quick, low-radiation scan that measures bone density,the standard test for osteoporosis risk after menopause.
References
1. National Institute on Aging (NIH). "What Is Menopause?",reports the average age of natural menopause in the US is 52, with most women beginning the transition between ages 45 and 55. https://www.nia.nih.gov/health/menopause/what-menopause
2. Avis NE, Crawford SL, Greendale GA, et al. "Duration of Menopausal Vasomotor Symptoms Over the Menopause Transition." JAMA Internal Medicine, 2015;175(4):531-539,the SWAN study; median total VMS duration of 7.4 years, persisting a median of 4.5 years after the final menstrual period. https://pmc.ncbi.nlm.nih.gov/articles/PMC4433164/
3. Study of Women's Health Across the Nation (SWAN). "Changes in Body Composition and Weight During the Menopause Transition" research summary,cites vasomotor symptom prevalence affecting up to 80% of women during the menopause transition. https://www.swanstudy.org/changes-in-body-composition-and-weight-during-the-menopause-transition/
4. Greendale GA, Karlamangla AS, Maki PM. "The Menopause Transition and Cognition." JAMA, 2020;323(15):1495-1496,review estimating that roughly 40–60% of women report cognitive difficulty ("brain fog") during the menopause transition. https://jamanetwork.com/journals/jama/articlepdf/2763134/jama_greendale_2020_it_200007.pdf
5. Greendale GA, Sternfeld B, Huang M, et al. "Changes in Body Composition and Weight During the Menopause Transition." JCI Insight, 2019;4(5):e124865,SWAN cohort data showing accelerated fat gain and lean mass decline around the final menstrual period, independent of chronological aging. https://insight.jci.org/articles/view/124865
6. The North American Menopause Society (NAMS). "The 2020 Genitourinary Syndrome of Menopause Position Statement." Menopause, 2020;27(9):976-992,reports GSM affects approximately 27% to 84% of postmenopausal women and is likely underdiagnosed and undertreated. https://www.menopause.org/docs/default-source/default-document-library/2020-gsm-ps.pdf
Citations are provided for major statistics referenced in this article. As with all medical literature, individual study populations and methods vary; your physician can help interpret how this evidence applies to your specific situation.

 Meet Your Doctor
Meet Your Doctor
Leave a Comment